The Vestibular System: Form and Function
- Ben O'Shannessy
- Nov 14, 2025
- 4 min read
When we look at the causes for dizziness and vertigo, the vestibular system is a crucial focus of our assessment. Many of the causes for vertigo originate from the vestibular system, but what exactly is it? Let's take a look.
The Purpose of the Vestibular System
The vestibular system is primarily responsible for the estimation of body position and motion. The input that comes to the vestibular system can originate from the inner ear (the vestibular apparatus above), from position sensation (what we would term as proprioception, visual signals and intended movements (motor commands and conscious movements initiated by us) (1).
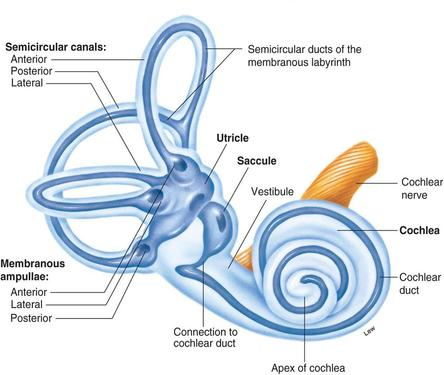
The peripheral sensory apparatus (vestibular apparatus) is one half of the inner ear. It is located deep behind the ear, encased in the bone of the skull for protection. It is divided into 2 parts. The bony labyrinth, which is the outer structure of the vestibular apparatus and the membranous labyrinth, which houses the internal part containing the organs responsible for sensation. These are the three semircular canals, and the two otoliths organs (as well as their crystals, which i've spoken about here). Running through them is something called endolymphatic fluid, which shifts with head movement. At specific locations throughout there are strategically placed hair cells, which are responsible for detecting motion and turning it into a signal the body can use for balance.
The Semicircular Canals
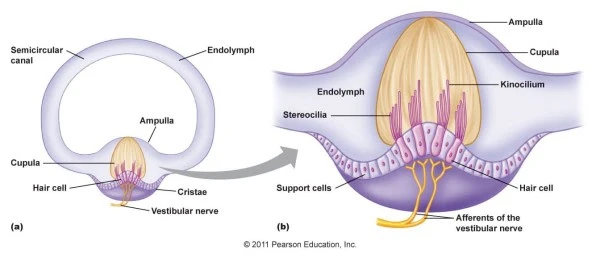
The semicircular canals (SCCs) are mainly responsible for detecting head velocity. This means any angular head movement, such as nodding or turning the head. The movement of the fluid within them stimulates a small membrane at one end called the cupula, which subsequently causes movement of the associated hair cells, measuring the movement. The cupula is only stimulated by movement, and it's motion is directly proprortionate to the amount of head movement there is.
The Otoliths
These two fellows are responsible primarily for detection of gravity, and pick up the stimulus of acceleration and deceleration. Movements such as forward and back, up and down and tilting are detected, which makes the otoliths responsible for our ability to feel the acceleration of a car or aeroplane, or to feel the elevator speed up or slow down. They won't detect constant speed however, which is why when the cruise control is on, there is less sensation of movement.
To sense gravity, there must be some weight. That's where the crystals come in. The crystals, or otoconia, are attached the otoliths and provide weight that moves with gravity allowing for sensation. For a more detailed description, have a read here.

The Vestibular System as a Balance Organ
As a system, the two ears work together. Turning of the head causes changes in the firing rate of the ear, which in turn gives us a sense of motion. The system is always active. At rest, it will fire somewhere between 70-100Hz, averaging around 90Hz (1Hz is one cycle per second, so it's firing around 90 times a second) (2, 3). The important part here is that both ears are firing equally. If we turn the head, the rate of the ear towards which we've turned goes up, and the opposite ear goes down. This difference creates a perception of movement. As soon as the head stops moving, these return to an equal resting rate.
What happens when motion is detected?
When the head is moved, the signal is detected by the small movements of the hair cells. These hair cells turn the mechanical motion into an electrical signal, which is sent along the vestibular nerve to the brain. This allows for the function of three reflexes:
The Vestibulo-Ocular Reflex: This is the link between the ear and the eyes. It uses the signal from the ear to match eye speed to head speed, effectively allowing you to maintain stable vision during head movement.
The Vestibulo-Spinal Reflex: This controls the response of the spinal muscles to stabilise the body during movement.
The Vestibulo-Collic Reflex: Acts on the neck muscles to stabilise the head.
What happens when things go wrong?
When there are abnormalities with the vestibular function, it can come in two forms - hyperactivity or hypoactivity. Looking at it this way is a little both simplistic, but it's useful for a general idea.
Hyperactivity is often when we see vertigo occur. This is when there is an artificial stimulus or imbalance between the ears. This can happen with conditions such as:
Benign Paroxysmal Positional Vertigo (where otoconia displacement causes overstimulation with movement)
Meniere's disease (where fluid changes within the ear will increase the activity of of an ear, creating an imbalance)
Vestibular neuritis (which has the opposite effect, restricting the signal of the nerve of one ear and effectively turning it off, so there is an imbalance in the other direction).
When look at a hyPOactivity of the vestibular system, or a hypofunction, it means the system is not working fast enough. As a result we tend to see the system not keep up with the head movement, not providing an adequate signal to allow the reflexes to work (4, 5). This means the eyes can't compensate for the head movement resulting in unstable vision, and our neck and spine movements struggle with stability.
References
Herdman, S and Clendaniel, R, 2014, Vestibular Rehabilitation, Anatomay and Physiology of the Normal Vestibular System, FA Davis
McElvain et al, 2015, Implementation of linear sensory signaling via multiple coordinated mechanisms at central vestibular nerve synapses, Neuron, Vol. 19(85), pp. 1132–1144
Gittis, AH, Moghadam, SH and du Lac, S, 2010, Mechanisms of Sustained High Firing Rates in Two Classes of Vestibular Nucleus Neurons: Differential Contributions of Resurgent Na, Kv3, and BK Currents, Journal of Neurophysiology, vol. 104(3), pp. 1625–1634
Strupp et al, 2017, Bilateral vestibulopathy: diagnostic criteria Consensus document of the Classification Committee of the Bárány Society, Journal of Vestibular Research, vol. 27, pp. 177–189
Lucieer et al, 2018, Full spectrum of reported symptoms of bilateral vestibulopathy needs further investigation—a systematic review, Frontiers in Neurology, vol. 9, pp. 352.



Comments